ACEs Risk & Protective Factors and the Social Ecological Model
Understanding and preventing ACEs is possible but complex. ACEs often occur due to multiple individual, family, and community risks, and can be buffered by multiple protective factors.
The Social-Ecological Model (SEM) can help us name and address the factors that put children at risk for experiencing ACEs from all levels—we call these risk factors. Incorporating them into data collection and monitoring systems can help guide our research and public health practice, and help us understand which individuals, communities, and subgroups are most likely to experience ACEs. That way, we can focus prevention efforts where ACEs are more likely to occur.
While risk factors make a child more likely to experience ACEs, protective factors make a child less likely to experience ACEs. Protective factors also reduce the impact of ACEs among children who experience ACEs. It is important to know that even beyond their ability to prevent and reduce the impact of ACEs, protective factors promote children’s health, development, well-being, and opportunities. We can categorize protective factors according to the SEM, as well.
| RISK FACTORS | PROTECTIVE FACTORS | |
|---|---|---|
| INDIVIDUAL Example: | Belief in the acceptability of corporal punishment | Living in stable housing |
| RELATIONSHIP Example: | Adults in a child's life who are under economic stress | Adults in a child's life work through conflicts peacefully and calmly |
| COMMUNITY Example: | Living in a community where food insecurity is prevalent | Living in a community with few abandoned or vacant buildings and low rates of violence |
| SOCIETAL Example: | Living in a society that views violence as acceptable or inevitable | Living in a society where public policy supports high-quality and affordable early childhood education |
Social Determinants of Health (SDOH) and ACEs
In addition to the SEM, Social Determinants of Health (SDOH) is another framework that can inform ACEs data collection and monitoring, as well as efforts to collect and monitor data for PCEs.
Social determinants of health are the nonmedical factors that influence health outcomes. They are the conditions in which people are born, grow, work, live, and age, and the wider set of forces and systems that shape conditions of daily life.
The Social Determinants of Health can be placed into five domains, which include economic stability, educational access and quality, healthcare access and quality, neighborhood and built environment, and social and community context.
When we consider the SDOH in our data collection and monitoring efforts, we can better identify the conditions that place some communities, their families, and children at greater risk for experiencing ACEs. This can help us better identify where to invest prevention, intervention, and response efforts to improve conditions and supports for communities that have fewer resources to ensure that all children and families can thrive.
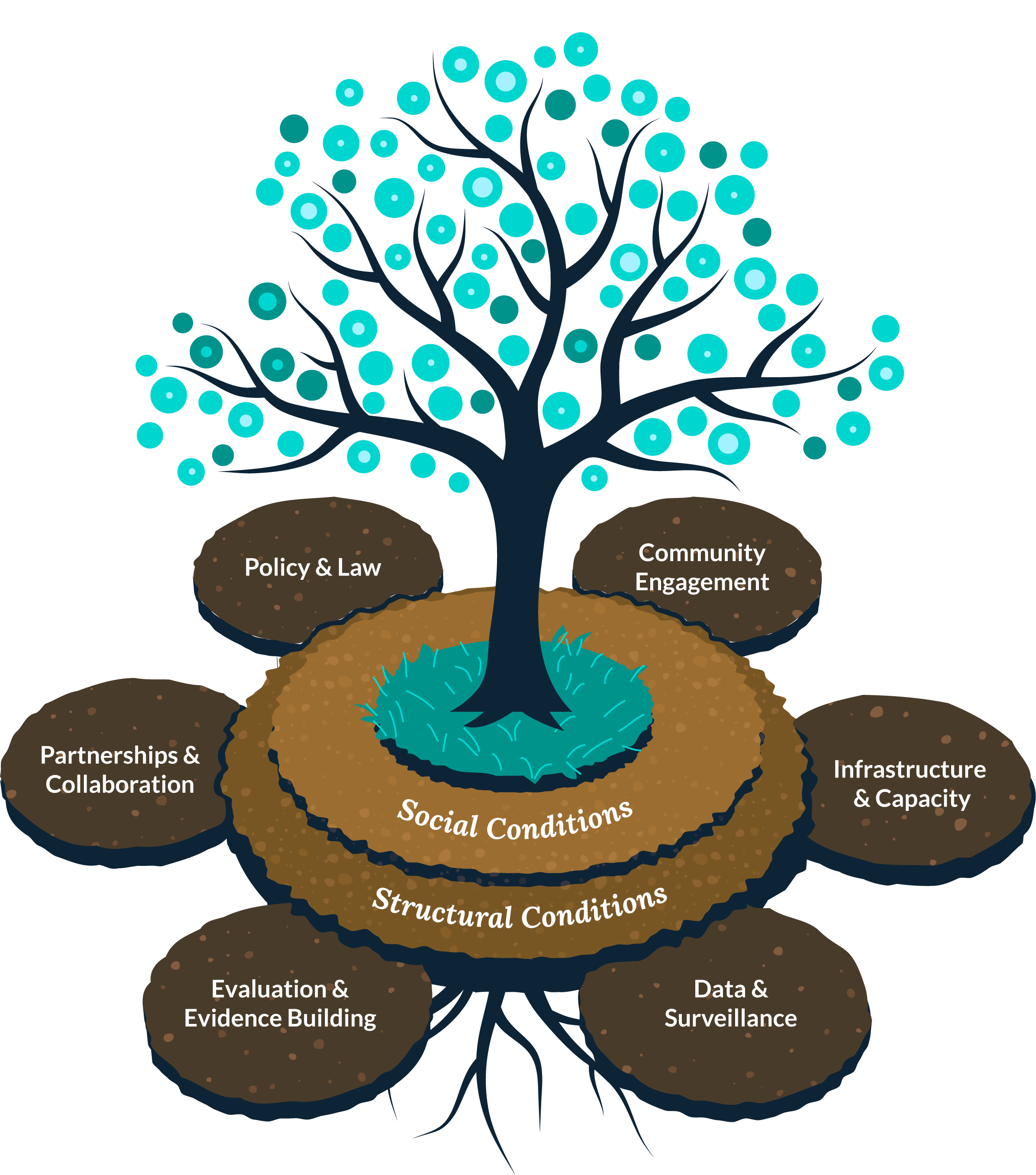
Tree diagram illustrating a comprehensive framework with multiple components: The image shows a stylized tree with a dark trunk and branches extending upward, adorned with numerous teal/turquoise circular dots representing leaves or fruit.
Root system and foundational layers: The tree grows from a layered foundation consisting of:
- Bottom layer (darkest): "Structural Conditions"
- Middle layer: "Social Conditions"
- Top layer (around the tree base): Teal/turquoise area where the tree trunk emerges
Six oval-shaped components surrounding the foundation:
- Top left: "Policy & Law"
- Top right: "Community Engagement"
- Middle right: "Infrastructure & Capacity"
- Bottom right: "Data & Surveillance"
- Bottom left: "Evaluation & Evidence Building"
- Middle left: "Partnerships & Collaboration"
The tree's root system extends beneath all components, suggesting these six areas are interconnected and supported by the foundational social and structural conditions. The flourishing tree crown with abundant teal dots represents the positive outcomes when all these elements work together effectively.
Just as we compare ACEs and PCEs to the weeds, sunlight, and water which affect a seedling’s ability to grow and thrive, we can think of the SDOH as the seedling’s soil.
The quality of that soil affects ACEs, PCEs, and health outcomes.
Including Positive Childhood Experiences (PCEs) in Data Collection Efforts
Positive childhood experiences (PCEs) are a subset of protective factors which reflect the child’s subjective, reported experience. For example, “living in a community with access to green spaces” may be a community-level protective factor that you can measure without a child’s input by counting the number of parks in a community. And if a child reports, “I frequently use the park in my neighborhood and feel safe there,” that is a PCE.
Consider identifying PCEs that align with the prevention, intervention, and response strategies that you are implementing so that you can monitor whether they are having the intended impact in your jurisdiction.
Instructions: Click Next to learn more about the relationship between ACEs, PCEs, and Health Outcomes

Image 1 of 3: Basic ACE Model
A conceptual diagram showing the relationship between childhood experiences and health outcomes. The diagram features three main circular elements connected by arrows and dotted lines:
- Positive Childhood Experiences (gray circle, top center): Connected by a gray dotted arrow pointing down toward the adverse experiences circle
- Adverse Childhood Experiences (purple circle, bottom left): Surrounded by purple virus-like symbols with spikes. Connected by a solid black arrow pointing right to health outcomes
- Health Outcomes (purple circle, bottom right): Accompanied by a flourishing tree with purple circular dots representing leaves or fruit
This image illustrates the basic model where adverse childhood experiences directly impact health outcomes, while positive childhood experiences are shown as a separate, less integrated factor.
When we don’t prevent potentially traumatic experiences in childhood, such as experiencing or witnessing violence in the home, school, or community, these traumatic experiences can lead to negative health outcomes.

Image 2 of 3: Enhanced Model with Protective Factors
An enhanced version of the previous model showing how positive childhood experiences can intervene in the relationship between adverse experiences and health outcomes. The diagram includes:
- Positive Childhood Experiences (yellow circle, top center): Now highlighted in yellow, showing two pathways labeled "Prevention Effect" (solid arrow to adverse experiences) and "Direct Impact" (solid arrow to health outcomes)
- Adverse Childhood Experiences (now gray circle, bottom left): Still surrounded by virus-like symbols, connected to health outcomes by a gray arrow
- Health Outcomes (teal circle, bottom right): Now in teal color, still accompanied by the flourishing tree with teal circular dots
- Mitigating Effect (small blue circle in center): Connected by a dotted line from positive experiences, showing an additional protective pathway
This model demonstrates that positive childhood experiences can prevent adverse experiences, directly improve health outcomes, and provide mitigating effects even when adverse experiences occur.
Science suggests that PCEs may work in three ways. First, positive childhood experiences can prevent ACEs from happening in the first place. Second, they can directly produce positive health outcomes. Finally, positive childhood experiences can also lessen the negative effects of ACEs.

Image 3 of 3: Complete Integrated Model
The final model showing the full integration of positive and adverse childhood experiences in determining health outcomes. This version includes:
- Positive Childhood Experiences (yellow circle, top center): Maintains the same yellow highlighting and two pathways as Image 2
- Adverse Childhood Experiences (purple circle, bottom left): Returns to purple coloring, emphasizing its continued significance in the model
- Health Outcomes (teal circle, bottom right): Remains teal, with the flourishing tree representing positive health outcomes
- Mitigating Effect (blue circle in center): Shows the ongoing protective influence of positive experiences
This complete model illustrates that both positive and adverse childhood experiences are significant factors in health outcomes, with positive experiences serving multiple protective roles through prevention, direct benefits, and mitigation of adverse effects.
ACEs can lead to negative health outcomes—increased risk for illness, disease, and death in the short- or long-term. PCEs are necessary for positive health outcomes in the short- or long-term, and they can also mitigate the negative effects of ACEs.
Most scientific research about PCEs focuses on the importance of positive relationships between children and their parents, caregivers, friends, and mentors. However, there are a lot of other important PCEs, too, including those that focus on children having safe and stable environments and opportunities to find activities that bring them joy and connection.
Ongoing research suggests PCEs may have exciting implications for interventions that don’t just prevent ACEs and lessen their effects—they can also directly produce better health as independent and profound determinants of positive health outcomes. PCEs data collection is essential for monitoring the population-level impact of efforts to promote better early and long-term health outcomes.
![]() Learn MoreIn this module, you’ll explore how data collection and monitoring helps identify disparities and informs focused interventions.
Learn MoreIn this module, you’ll explore how data collection and monitoring helps identify disparities and informs focused interventions.